The Addiction Epidemic: Re-ordering Strategies for Substance Abuse Disorders from Intervention to Prevention
More than 64,000 Americans died from drug overdoses in 2016, including illicit drugs and prescription opioids…nearly double in a decade. An estimated 88,000 people (approximately 62,000 men and 26,000 women) died from alcohol abuse in the same year. We lost 152,000 people. This makes alcohol and drug abuse/addiction the third leading preventable cause of death in the United States. Only heart disease and cancer took more lives.Congress approved and the President signed a bill funding $7.4 billion for addiction in 2018. But are we allocating our resources well? Are we addressing this health crisis in new and effective ways? It is a good and meaningful try to be sure. The problem is that we continue to allocate much more money and effort into putting out fires as opposed to preventing them.

Chattooga River
Are We Focused on the Real Problem? Insights from the Chattooga River
In my role as an addiction professional, I used to speak before groups of mental health, substance abuse and adolescent treatment providers on a fairly regular basis. One of the stories I liked to tell is that of a hiker in the Blue Ridge Mountains who had wandered onto an active emergency situation at a Class IV rapid on the Chattooga River.
There were ambulances, EMT’s, police officers, a coroner and lots of onlookers trying desperately to pull the dead and dying from still-treacherous waters below the rapids. The victims were young people who were beaten by rocks, lungs full of river, no longer able to help themselves. Knowing that he would only get in the way, the hiker hustled upstream. There he found another frantic situation indeed.
The whitewater of Bull Sluice was enveloping kayaks, canoes and swimmers. Specially trained First Responders and Experienced Whitewater Guides were using all of their skills in efforts to get people out of harm’s way to little avail. So the hiker went around the bend and up to a point where he heard cries for help and found several river guides and volunteers throwing floating devices on ropes, wading into swift water, hauling kids and boats up to shore from an area just above the Class IV treachery. Many were being rescued but some were swept away.
There was still little room for him to be of any use, so the hiker ran along the bank to find a group of youngsters swimming in the river. Some neighbors and volunteers from the down river site were trying to talk them into getting out of the water…warning of the perils downstream.
Several of them paid attention and followed the urgings of their warnings and headed in for dry land. Finally, a few hundred yards further on, the hiker found a bend in the river where it seemed to be warm and inviting. A group of kids were changing into swim wear and heading toward the water with rafts and inner tubes. There were no adults supervising, warning or rescuing. The situation was so ostensibly innocent.
He approached the young people, told them of all he had witnessed and talked about finding another way to enjoy the afternoon that might not be so life-threatening. He showed them the way to a little private cove where still water, a diving well and nice beach waited. Everyone took him up on the offer and enjoyed a safe day of adventure.
From the Intensive Care to Early Screening:
Our Inverted Focus (or Looking for Cures in All the Wrong Places)
I think my subtitle is a little cutesier than it should be. It makes me think of the 1980 Country song “Lookin’ for Love” by Johnny Lee making it hard to resist. Anyway, my story about the Blue Ridge Hiker is what I believe is an upside-down pyramid of attention, emphasis, funding and research in dealing with the opioid/addiction epidemic. The following are the categories of treatment intervention as I have experienced them in decades of direct service in the field of Substance Abuse Disorders (SUDs).Tertiary Intervention: Most of our precious time and resources has been given to what I call tertiary intervention. Like the hiker approaching the chaotic rescue efforts downriver, we have spent most of our time giving CPR to the dying and burying the others. Tertiary Interventions include;
- Emergency Response Teams (First Responders, LEO’s, Emergency Rooms, Hospitals, Intensive Care)
- 24 hour hospital based Short Term Medical Detox Centers
- Criminal Justice System
- Universal availability of naloxone
Secondary Intervention: These are Medically Managed Services for adolescents and adults. In my story, it is the discovery of direct whitewater rescue. Secondary Interventions include;
- Hospital based 24-hour nursing care and daily physician care for severe, unstable patients who cannot manage life without these intensive services.
- 24 hour Intensive Inpatient Services Withdrawal Management centers with counseling, physician, nursing and medication management services.
- Residential treatment centers with flexible programs to meet individual treatment needs depending on severity of illness.
Primary Intervention: Services at this level help those who do not require round-the-clock care. The hiker in the little tale finds swimmers and adventurers above the rapids but in some degree of real trouble. Primary Interventions include;
- Partial Hospitalization Services for adolescents and adults, this level of care typically provides 20 or more hours of service a week.
- Intensive Outpatient Services for adolescents and adults, this level of care typically consists of 9 or more hours of service a week.
- Outpatient Services for adolescents and adults, this level of care typically consists of less than 9 hours of service a week.
- Opioid Treatment Programs. (OTP) utilizes methadone or buprenorphine formulations in an organized, ambulatory, addiction treatment clinic for clients with severe Opioid-Use Disorders to establish a maintenance state of addiction recovery
- Drug Courts
Primary Prevention: Early Intervention for Adults and Adolescents, this level of care constitutes a service for individuals who, for a known reason, are at risk of developing substance-related problems, or a service for those for whom there is not yet sufficient information to document a diagnosable substance use disorder. This represents the final stop for our hiker. Primary Preventions include;
- Adverse Childhood Experience Screening (ACE’s)
- Classroom based substance abuse education programs
- Strategic Prevention Framework by SAMHSA
- Recovery Community Services Programs. Organizations that are grassroots, separate from the government run programs, separate from treatment services i.e., Faces and Voices of Recovery (FAVOR)
- Prescription Drug Monitoring Programs (PDMP). An electronic database that tracks controlled substance prescriptions in a state. PDMPs can provide health authorities timely information about prescribing and patient behaviors that contribute to the epidemic and facilitate a nimble and targeted response.
There is practically universal accord that our methods of dealing with drug and alcohol abuse have failed to achieve the desired results. The efforts to stem the tide of addiction by declaring a war on drugs (which was really a war on people engaged in it) proved almost fruitless.The problem is that despite good intentions, and an allocation of massive funding, we are continuing to pour resources into the least effective means of turning the tables on our nationwide epidemic. Policy makers and leaders have decided to ignore the facts and double down on a status quo method of dealing with a healthcare crisis which has been raging for almost 20 years. And the status quo has made virtually zero impact (statistically speaking) on outcomes.The Comprehensive Addiction and Recovery Act (CARA) of 2018 heralds a new era which will “Expand prevention and educational efforts—particularly aimed at teens, parents and other caretakers, and aging populations—to prevent the abuse of methamphetamines, opioids and heroin, and to promote treatment and recovery. However, it authorizes funding at the roughly the following levels nationwide;
- Inpatient, outpatient and OTP treatment at $4.1 billion
- Criminal Justice at $1.59 billion
- Prevention at $221 million (4.4 million per state)
- Recovery Support Services (FAVOR, recovery high schools, recovery housing) at $7 million or $140 thousand per state (not even enough to fund services in Upstate South Carolina for example)
 There is a place on the planet which has used effective local initiatives in the form of policies to discourage drug use while offering solid alternative programs. Iceland built an anti-drug plan that focuses largely on providing kids with after-school activities, from music and the arts to sports like soccer and indoor skating to many other clubs and activities.They coupled this approach with banning alcohol and tobacco advertising, enforcing curfews for teenagers, and getting parents more involved in their kids’ schools to further discourage drug use.Researcher Harvey Milkman says of Iceland’s approach, that it’s “a social movement around natural highs: around people getting high on their own brain chemistry … without the deleterious effects of drugs.”As a result, Iceland, which had one of the worst drug problems in Europe, has seen adolescent consumption fall. The number of 15 and 16 year-olds who got drunk in the previous month fell from 42 percent in 1998 to just 5 percent in 2016, and the number who ever smoked marijuana dropped from 17 percent to 7 percent in the same time frame. In a similar time period, from 1997 to 2012, the percentage of 15 and 16 year-olds who participated in sports at least four times a week almost doubled — from 24 to 42 percent — and the number of kids who said they often or almost always spent time with their parents on weekdays doubled, from 23 to 46 percent.[/et_pb_tab][et_pb_tab title="The Vermont Approach" _builder_version="3.0.101"]
There is a place on the planet which has used effective local initiatives in the form of policies to discourage drug use while offering solid alternative programs. Iceland built an anti-drug plan that focuses largely on providing kids with after-school activities, from music and the arts to sports like soccer and indoor skating to many other clubs and activities.They coupled this approach with banning alcohol and tobacco advertising, enforcing curfews for teenagers, and getting parents more involved in their kids’ schools to further discourage drug use.Researcher Harvey Milkman says of Iceland’s approach, that it’s “a social movement around natural highs: around people getting high on their own brain chemistry … without the deleterious effects of drugs.”As a result, Iceland, which had one of the worst drug problems in Europe, has seen adolescent consumption fall. The number of 15 and 16 year-olds who got drunk in the previous month fell from 42 percent in 1998 to just 5 percent in 2016, and the number who ever smoked marijuana dropped from 17 percent to 7 percent in the same time frame. In a similar time period, from 1997 to 2012, the percentage of 15 and 16 year-olds who participated in sports at least four times a week almost doubled — from 24 to 42 percent — and the number of kids who said they often or almost always spent time with their parents on weekdays doubled, from 23 to 46 percent.[/et_pb_tab][et_pb_tab title="The Vermont Approach" _builder_version="3.0.101"]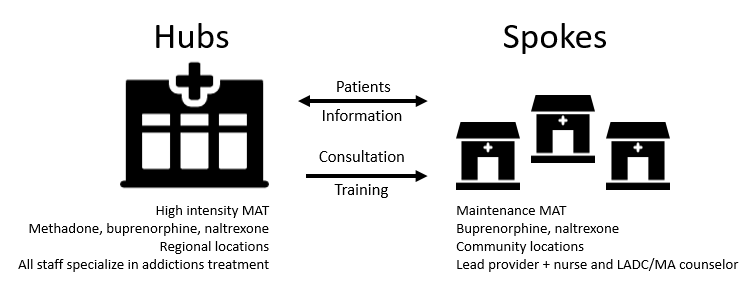 In another approach, the State of Vermont has developed a comprehensive health care policy which has changed the outcomes for opioid disorders dramatically using medication assisted treatment programs.It is called the “hub and spoke model” which was developed by the American Society of Addiction Medicine. The results have been encouraging. Vermont is doing much better than nearby states.It was the only state in New England that in 2015 was below the national average (of 16.3 per 100,000 people) for drug overdose deaths.[/et_pb_tab][et_pb_tab title="The Los Angeles Approach" _builder_version="3.0.101"]
In another approach, the State of Vermont has developed a comprehensive health care policy which has changed the outcomes for opioid disorders dramatically using medication assisted treatment programs.It is called the “hub and spoke model” which was developed by the American Society of Addiction Medicine. The results have been encouraging. Vermont is doing much better than nearby states.It was the only state in New England that in 2015 was below the national average (of 16.3 per 100,000 people) for drug overdose deaths.[/et_pb_tab][et_pb_tab title="The Los Angeles Approach" _builder_version="3.0.101"] One of the most dramatic approaches to dealing with the Drug Crisis can be found at Homeboy Industries in Los Angeles. Here, and in a multitude of spin-off organizations, comprehensive employment and life redirection strategies have been used to help gang members, previously incarcerated individuals and families to overcome violence and addiction.They are unconventional. Established by Rev. Gregory Boyle, they tell that at Homeboys, hope has an address. He tells us that, “Homeboy Industries has been the tipping point to change the metaphors around gangs and how we deal with them in Los Angeles County.This organization has engaged the imagination of 120,000 gang members and helped them to envision an exit ramp off the "freeway" of violence, addiction and incarceration. And the country has taken notice. We have helped more than 40 other organizations replicate elements of our service delivery model, broadening further the understanding that community trumps gang -- every time.”Every member of Homeboys must test clean on drug screens to be a part of the community service. Their unusual program is based on a spiritual model of unconditional love.[/et_pb_tab][et_pb_tab title="The Memphis Approach" _builder_version="3.0.101"]Memphis is using ACE’s.
One of the most dramatic approaches to dealing with the Drug Crisis can be found at Homeboy Industries in Los Angeles. Here, and in a multitude of spin-off organizations, comprehensive employment and life redirection strategies have been used to help gang members, previously incarcerated individuals and families to overcome violence and addiction.They are unconventional. Established by Rev. Gregory Boyle, they tell that at Homeboys, hope has an address. He tells us that, “Homeboy Industries has been the tipping point to change the metaphors around gangs and how we deal with them in Los Angeles County.This organization has engaged the imagination of 120,000 gang members and helped them to envision an exit ramp off the "freeway" of violence, addiction and incarceration. And the country has taken notice. We have helped more than 40 other organizations replicate elements of our service delivery model, broadening further the understanding that community trumps gang -- every time.”Every member of Homeboys must test clean on drug screens to be a part of the community service. Their unusual program is based on a spiritual model of unconditional love.[/et_pb_tab][et_pb_tab title="The Memphis Approach" _builder_version="3.0.101"]Memphis is using ACE’s.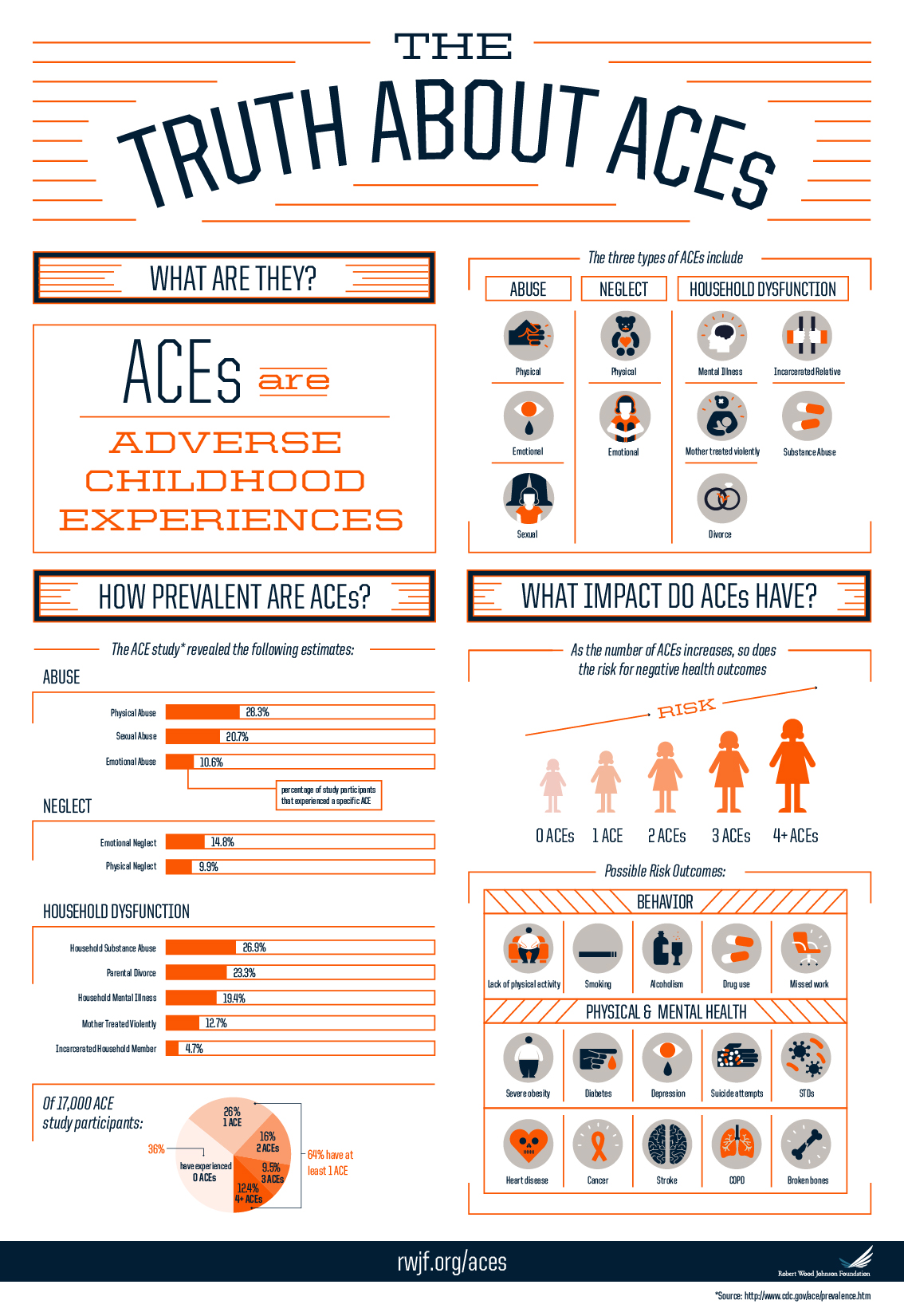 The Adverse Childhood Experiences (ACE) Awareness Foundation of Memphis “informs the community about the role of emotional trauma in mental, physical, and behavioral health, and implements innovative models that provide preventable and sustainable solutions to reducing toxic stress in family systems.The Foundation launched and provides strategic oversight to the ACE Task Force of Shelby County, the Universal Parenting Places, and the Parenting Support Warm Line.” Although not an addiction or substance abuse disorder specific program, ACE’s used in the comprehensive way Memphis is developing will stem the tide through screening and direct services. The fact is that pain drives addiction and SUDS. Drugs and alcohol are abused by people who have childhood experiences and trauma that the rest of us cannot imagine.They are seeking relief and a hiding place. When a community like Memphis gathers its schools, juvenile justice system, LEO’s, pediatricians, colleges, churches, other human service providers, parents and families together, you can be sure that something incredible will happen.There is new research telling us incredible things about the way addicted brains work. Drugs have been found to hijack dopamine systems making ‘getting high’ an almost unavoidable consequence. Also, the adolescent brain, when exposed to drug use has little chance to form good cognitive processes. The idea that addiction is a moral failing has been practically eliminated. With that in mind, it is even more important that we begin thinking outside of the box.[/et_pb_tab][/et_pb_tabs][et_pb_text _builder_version="3.0.101"]
The Adverse Childhood Experiences (ACE) Awareness Foundation of Memphis “informs the community about the role of emotional trauma in mental, physical, and behavioral health, and implements innovative models that provide preventable and sustainable solutions to reducing toxic stress in family systems.The Foundation launched and provides strategic oversight to the ACE Task Force of Shelby County, the Universal Parenting Places, and the Parenting Support Warm Line.” Although not an addiction or substance abuse disorder specific program, ACE’s used in the comprehensive way Memphis is developing will stem the tide through screening and direct services. The fact is that pain drives addiction and SUDS. Drugs and alcohol are abused by people who have childhood experiences and trauma that the rest of us cannot imagine.They are seeking relief and a hiding place. When a community like Memphis gathers its schools, juvenile justice system, LEO’s, pediatricians, colleges, churches, other human service providers, parents and families together, you can be sure that something incredible will happen.There is new research telling us incredible things about the way addicted brains work. Drugs have been found to hijack dopamine systems making ‘getting high’ an almost unavoidable consequence. Also, the adolescent brain, when exposed to drug use has little chance to form good cognitive processes. The idea that addiction is a moral failing has been practically eliminated. With that in mind, it is even more important that we begin thinking outside of the box.[/et_pb_tab][/et_pb_tabs][et_pb_text _builder_version="3.0.101"]
It’s Up to Us…Here and Now:
Just think…152,000 people lost from this preventable disease or disorder. People in our lives will die. We have a lot of work to do. Funding and programs will only go so far. Certainly, we have to encourage a change in the way budgets are allocated.Prevention first…at the very top priority…is the best and most worthwhile model to embrace. We cannot keep repeating mistakes of the past and expect different outcomes. But there is a spiritual, community reality that we must embrace as a foundation for how we deal with the problem of addiction and substance abuse disorders.The one who suffers is not someone else but is each and every one of us. If we are going to get beyond all of this, there is no other way to look at it. Our wounds are shared. We are all in this together. Here and now, and in each and every moment, we should be asking the question ‘What can I do to help’.Then we will find an answer._________________________________Robert Kenneth Jones is an innovator in the treatment of addiction and childhood abuse.In a career spanning over four decades, his work helping people recover from childhood abuse and addiction has earned him the respect of his peers.His blog, An Elephant for Breakfast, testifies to the power of the human spirit to overcome the worst of life’s difficulties. We encourage you to visit and share this rich source of healing, inspiration and meditation.Contact Bob Jones on LinkedinBob Jones’ blog An Elephant for Breakfast[/et_pb_team_member][/et_pb_column][/et_pb_row][/et_pb_section]